Case Study of Low Blood Pressure
| ✅ Paper Type: Free Essay | ✅ Subject: Nursing |
| ✅ Wordcount: 1962 words | ✅ Published: 11 Sep 2017 |
- Mr Jones has a BP of 90/60. Please name the appropriate health terminology in relation to his BP. Normal Range =
Hypotension
Low blood pressure is referred to as hypotension, especially in the arteries of the systemic circulation. Hypotension is generally considered systolic blood pressure less than 90 millimetres of mercury (mmHg) or diastolic less than 60 mmHg.
A person’s blood pressure reading appears as two numbers. The first and higher of the two numbers is a measure of “systolic” pressure or the pressure in the person’s arteries when their heart beats and fills them with blood. The second number measures “diastolic” pressure or the pressure in the person’s arteries when their heart rests between beats.
A desired blood pressure is less than 120/80. In people who are considered to be healthy, low blood pressure without experiencing any symptoms is commonly not a concern and does not need to be treated. Low blood pressure may be a sign of an underlying issue, particularly in the elderly, where it might cause inadequate blood flow to their heart, vital organs, and brain.
Fortunately, chronic low blood pressure without symptoms is rarely serious. Health issues may happen, however, when a person’s blood pressure suddenly drops and their brain is deprived of an adequate blood and oxygen supply. The condition may lead to light-headedness or dizziness. A sudden drop in blood pressure usually happens in a person who has risen from a prone or sitting position to a standing one. When this occurs it is referred to as, ‘postural hypotension’ or ‘orthostatic hypotension’. Another type of low blood pressure may happen when a person stands for extended periods of time. This is referred to as, ‘neurally-mediated hypotension’.
Postural hypotension is considered to be a failure of a person’s cardiovascular system or nervous system to react appropriately to sudden changes. Usually, when a person stands up, some of their blood pools in their lower extremities. If this remains uncorrected, it would cause the person’s blood pressure to fall or decrease. A person’s body usually compensates by sending messages to their heart to beat faster and to their blood vessels to constrict, offsetting the drop in blood pressure. If this does not happen, or does not happen quickly enough, postural hypotension is the result.
Blood Pressure and Aging
The risk of low and high blood pressure commonly increases as a person ages due in part to changes during the aging process. The flow of blood to a person’s heart muscle and brain declines as a person ages, many times as a result of plaque build-up in their blood vessels. While the causes of low blood pressure may not always be clear, it might be associated with things such as:
- Heart arrhythmias
- Heart failure
- Heat exhaustion or heat stroke
- Hormonal issues such as an under-active thyroid, diabetes, or low blood sugar
- Liver disease
- Pregnancy
- Some over-the-counter drugs
- Some prescription medications
- Widening of the blood vessels
Causes of Sudden Drops in Blood Pressure
Sudden drops in a person’s blood pressure may be life-threatening. A number of different things may cause this type of hypotension. The causes of sudden drops in blood pressure may include:
- A reaction to alcohol or medication
- Anaphylaxis, a severe allergic reaction
- Heart muscle disease
- High body temperature
- Loss of blood
- Low body temperature
- Sepsis
- Severe dehydration from diarrhoea, vomiting, or fever
People at Risk of Postural Hypotension
Postural hypotension, or low blood pressure when a person stands up quickly, may happen to anyone for a number of reasons such as lack of food, dehydration, or simply being overly fatigued. It might also be influenced by a person’s genetic make-up, medication, aging, psychological factors, dietary ones, or acute triggers such as allergy or infection. Postural hypotension happens most often in people who are taking medications to control high blood pressure or, ‘hypertension’. It may also be related to strong emotions, pregnancy, diabetes, or hardening of a person’s arteries. Seniors are affected by postural hypotension in particular, especially seniors who experience high blood pressure or autonomic nervous system dysfunction.
Hypotension after eating is a common cause of dizziness or even falls.
It is most common after large meals containing a lot of carbohydrates. Medical science believes it is caused by blood pooling into a person’s vessels in their stomach and intestines. A number of medications are associated with postural hypotension as well. The medications may be divided into two major categories:
Medications used to treat high blood pressure such as beta-blockers, diuretics, calcium-channel blockers, and angiotensin-converting enzyme (ACE) inhibitors
Medications that have hypotension as a side effect such as anti-psychotics, neuroleptics, nitrates, anti-anxiety agents, tricyclic antidepressants, sedative-hypnotics, and medications for Parkinson’s disease
Some causes of naturally occurring postural hypotension exist.
For example, dehydration and electrolyte loss might result from vomiting, diarrhoea, excessive blood loss during menstruation, or other conditions. A person’s age associated decline in blood pressure regulation is another example and is something that might worsen due to certain health conditions or medications. Some diseases may cause postural hypotension as well. Diseases such as Shy-Drager syndrome or, ‘multiple system atrophy,’ nerve issues such as peripheral neuropathy or autonomic neuropathy, cardiovascular disorders, nutritional diseases, or alcoholism may cause postural hypotension.
Blood Pressure Ranges
Listed below are the ranges for Low (Table 1) Normal (Table 2) and High (Table 3) blood pressure respectively.
|
Systolic pressure (mm Hg) |
Diastolic pressure (mm Hg) |
Pressure Range |
|
90 |
60 |
Borderline Low blood Pressure |
|
60 |
40 |
Too Low Blood Pressure |
|
50 |
33 |
Dangerously Low Blood Pressure |
Table 1 Low Blood Pressure Range
|
Systolic pressure (mm Hg) |
Diastolic pressure (mm Hg) |
Pressure Range |
|
130 |
85 |
High Normal Blood Pressure |
|
120 |
80 |
Normal Blood Pressure |
|
110 |
75 |
Low Normal Blood Pressure |
Table 2 Normal Blood Pressure Range
If one or both numbers are usually high, you have high blood pressure (Hypertension).
|
Systolic pressure (mm Hg) |
Diastolic pressure (mm Hg) |
Stages of High Blood Pressure |
|
210 |
120 |
Stage 4 |
|
180 |
110 |
Stage 3 |
|
160 |
100 |
Stage 2 |
|
140 |
90 |
Stage 1 |
Table 3 High Blood Pressure Range
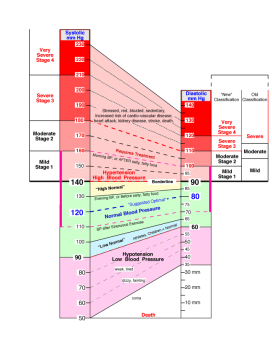
Figure 1Visual representation of Systolic and Diastolic Ranges
|
Age |
Systolic BP |
Diastolic BP |
|
3-6 |
116 |
76 |
|
7-10 |
122 |
78 |
|
11-13 |
126 |
82 |
|
14-16 |
136 |
86 |
|
17-19 |
120 |
85 |
|
20-24 |
120 |
79 |
|
25-29 |
121 |
80 |
|
30-34 |
122 |
81 |
|
35-39 |
123 |
82 |
|
40-44 |
125 |
83 |
|
45-49 |
127 |
84 |
|
50-54 |
129 |
85 |
|
55-59 |
131 |
86 |
|
60+ |
134 |
87 |
The average Systolic and Diastolic blood pressure is affected by age, as shown in
|
Age |
Males (mmHg) |
Females (mmHg) |
|
1 – 3 |
80/34 – 120/75 |
83/38 – 117/76 |
|
4 to 6 |
88/47 – 128/84 |
88/50 – 122/83 |
|
7 – 10 |
92/53 – 130/90 |
93/55 – 129/88 |
Table 4 Average Systolic and Diastolic Ranges of Neonates and Infants
Table 5 Average Systolic and Diastolic Ranges of Children and Adults
- Mr Jones has a HR of 153. Please name the appropriate health terminology in relation to his HR reading. Normal Range =
What is an arrhythmia?
An arrhythmia is a disruption in the heart’s normal electrical system which causes an abnormal or irregular heart beat for no apparent reason. Anyone can develop an arrhythmia, even a young person without a previous heart condition. However, arrhythmias are most common in people over 65 who have heart damage caused by a heart attack, cardiac surgery or other conditions. There are many types of arrhythmias, including:
•Heartbeats that are too slow (bradycardia)
•Heartbeats that are too fast (tachycardia)
•Extra beats
•Skipped beats
•Beats coming from abnormal areas of the heart
Typical symptoms
Some arrhythmias may occur without any symptoms. Others may cause noticeable symptoms, such as:
•Chest pain
•Dizziness, sensation of light-headedness
•Fainting
•Fatigue
•Sensation of a missed or extra heart beat
•Sensation of your heart fluttering (palpitations)
•Shortness of breath
•Weakness
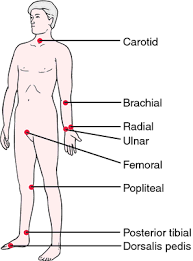
Figure 2 Location of Arterial Pulses where Heart Rate can be Detected

Figure 3 Normal Heart Rate on an ECG
Symptoms of Arrhythmias
Symptoms of arrhythmias can vary widely from person to person. An arrhythmia may last for a few minutes, a few hours, a few days, even a few weeks at a time. Some people feel no symptoms at all. Most commonly, patients report feeling a rapid heartbeat, often described as a “fluttering” sensation. Depending on the severity of the arrhythmia, that may be the only symptom experienced. Others may experience shortness of breath, fatigue, dizziness or fainting.
Types of Arrhythmias
Arrhythmias that cause heartbeats that are too fast are called tachycardia. There are several different types of tachycardia, which are categorized by where they originate in the heart.
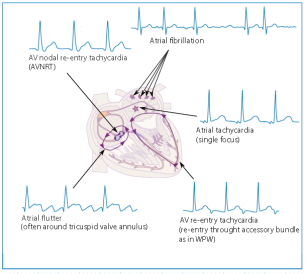
Figure 4 Supraventricular Tachycardia Location and ECG Presentation
- Supraventricular Tachycardia (SVT) is a general term describing any rapid heart rate originating above the ventricles (the lower chambers of the heart). The most common SVTs are described below.
- Atrial fibrillation (AF or AFib) is the most common SVT. During AF, the heartbeat produced by the atria is irregular and rapid, sometimes up to 4 times faster than normal. This impairs the heart’s ability to efficiently pump blood and increases the risk of developing blood clots which can cause a transient ischemic attack (TIA) or stroke.
- Atrial flutter (AFL) is similar to atrial fibrillation in that it is characterised by a rapid heartbeat, sometimes up to 4 times faster than normal that originates in the atria. It differs from atrial fibrillation (AF) in that the heartbeat is regular, not irregular. Atrial flutter also carries the risk of developing blood clots, though not as great as with AF. With atrial flutter, the electrical signal becomes “trapped” in the right atrium. It repeatedly travels in a circular pattern inside the right atrium, only occasionally “escaping” through the AV node to the ventricles. This causes your atria to beat faster than the ventricles of your heart, at rates between 150 and 450 beats each minute.
- Atrioventricular nodal re-entrant tachycardia (AVNRT) is the second most common SVT. In a normal heart, there is a single electrical pathway, or “gate”, called an atrioventricular node (AV node) that controls the timing and direction of the electrical signal as it travels from the upper chambers (atria) to the lower chambers (ventricles) of the heart. With AVNRT, an extra electrical pathway forms which allows the electrical signal to travel backward through the “gate” (AV Node) at the same time, starting another heartbeat. During AVNRT the electrical signals continuously go around the 2 pathways in a circular pattern called re-entry. This can lead to a very fast heart rate of 160 to 220 beats per minute.
- Atrioventricular reciprocating tachycardia (AVRT) is similar to AVNRT in that an extra electrical pathway is formed that allows the electrical signal to travel backward from the ventricles to the atria. However, in AVRT the extra pathway circumvents the AV node, or “gate”. This extra pathway around the outside of the AV node is called an accessory pathway.

- Ventricular Tachycardia (VT) is a rapid heart rate (160 to 240 beats per minute) that originates in the ventricles. It may cause the heart to become unable to pump adequate blood throughout the body. VT most often occurs in patients with underlying structural heart disease, such as ischemic heart disease.

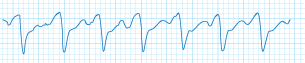
Figure 6Ventricular Fibrillation ECG Presentation
- Ventricular Fibrillation (VF) is a tachycardia which causes the ventricles to contract in an irregular and very rapid manner. The heart immediately loses its ability to pump blood throughout the body. VF causes immediate loss of consciousness, and is invariably fatal within minutes unless it is stopped (usually by using a defibrillator.)
|
AGE |
HEART RATE (BEATS/MIN) |
|
Infant |
120-160 |
|
Toddler |
90-140 |
|
Preschooler |
80-110 |
|
School-age child |
75-100 |
|
Adolescent |
60-90 |
|
Adult |
60-100 |
Table 6 Average Heart Rate Range by Age (Rested)


- Mr Jones has oxygen saturations of 75%. Please name the appropriate health terminology in relation to his oxygen saturations. Normal Range =
Pulse oximetry is a non-invasive and continuous method of determining the oxygen saturation of haemoglobin (SpO2). Peripheral oxygen saturation (SpO2) is usually measured with a pulse oximeter placed on the finger. SpO2 is normally 95% to 100%. If the level is below 90%, it is considered low, resulting in hypoxemia. Blood oxygen levels below 80% may compromise organ function, such as the heart and brain, and should be addressed promptly. Accurate SpO2 measurements may be difficult to obtain on patients who are hypothermic, receiving IV vasopressor therapy, or experiencing hypoperfusion and vasoconstriction.


Figure 9 Pulse Oximeter
|
Oxygen Saturation Levels |
|
|
Severity |
% Saturation |
|
None/Minimal |
95-100% |
|
Mild |
90-94% |
|
Moderate |
80-89% |
|
Severe |
<80% |
Table 7 Oxidation (SpO2) Levels
- Mr Jones has a RR of 6. Please name the appropriate health terminology in relation to his RR reading. Normal Range =
Slow Breathing (Bradypnoea)
A slow respiratory rate is usually significant at a rate of 8 or less per minute. Often this is an emergency and requires immediate therapy. Conditions causing bradypnoea are the ingestion of drugs (such as, alcohol, narcotics, sedative-hypnotics), increased intracranial pressure from trauma and haemorrhage (pressure on the respiratory centre), severe respiratory depression (that is, CO2 narcosis) and coma from any cause. It is seen in many pre-arrest and end-stage conditions.
Treatment
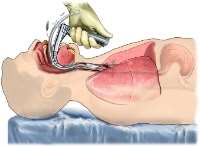
Assisted ventilation is often required with a bag-valve-mask (BVM). Endotracheal intubation is frequently necessary.



|
AGE RATE |
(BREATHS/MIN) |
|
Newborn |
35-40 |
|
Infant (6 months) |
30-50 |
|
Toddler (2 years) |
25-32 |
|
Child |
20-30 |
|
Adolescent |
16-20 |
|
Adult |
12-20 |
Table 8 Respiration Rate Range by Age
- Mr Jones has a temperature of 39 C. Please name the appropriate health terminology in relation to his temperature reading. Normal Range =
|
Measurement site |
||||
|
Mouth / Armpit |
Ear / forehead |
Rectum |
||
|
Low temperature |
< 35.8 â-¦C |
< 35.7 â-¦C |
< 36.2 â-¦C |
Consult a doctor |
|
Normal temperature |
35.9 – 37.0 â-¦C |
35.8 – 36.9 â-¦C |
36.3 – 37.5 â-¦C |
You are perfectly well |
|
Increased temperature |
37.1 – 37.5 â-¦C |
37.0 – 37.5 â-¦C |
37.6 – 38.0 â-¦C |
You should get some rest |
|
Light fever |
37.6 – 38.0 â-¦C |
37.6 – 38.0 â-¦C |
38.1 – 38.5 â-¦C |
Check your temperature regularly and rest |
|
Moderate fever |
38.1 – 38.5 â-¦C |
38.1 – 38.5 â-¦C |
38.6 – 39.0 â-¦C |
Check your temperature regularly. Consult a doctor if you get worse or if the fever lasts for more than three days |
|
High fever |
38.6 – 39.5 â-¦C |
38.6 – 39.4 â-¦C |
39.1 – 39.9 â-¦C |
Consult a doctor, especially if the fever lasts for more than one day |
|
Very high fever |
39.6 – 42.0 â-¦C |
39.5 – 42.0 â-¦C |
40.0 – 42.5 â-¦C |
Go to emergency ward of a hospital |
Table 9 Human Body Temperature Ranges
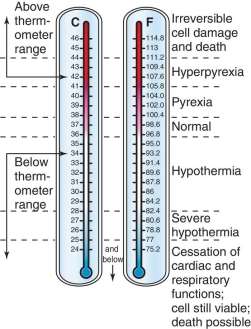
 Figure 12 Centigrade and Fahrenheit Representation of Temperature Ranges and Bodily Affection
Figure 12 Centigrade and Fahrenheit Representation of Temperature Ranges and Bodily Affection



- Please explain what the term dysphagia means in words that MR Jones can understand.
Dysphagia is another term for a swallowing disorder. A person with dysphagia may experience difficulty swallowing food, liquid and/or their saliva. Some people may be incapable of swallowing at all. Dysphagia occurs when there is a problem with any part of the swallowing process, and often is the result of a stroke. People with dysphagia often have to eat food which is softened and/or mashed and consume liquids which are thickened.
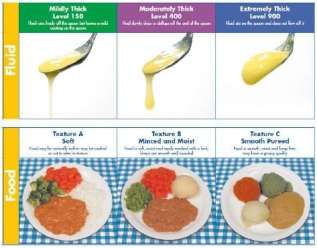
Figure 15 Fluid and Food for Dysphagic Persons
- Please describe hemiplegia as if you were explaining what this term meant to a family member of Mr Jones and how would this impact on taking his blood pressure?
What is hemiplegia?
Hemiplegia (sometimes called hemiparesis) is a condition that affects one side of the body. We talk about a right or left hemiplegia, depending on the side affected. It is caused by injury to parts of the brain that control movements of the limbs, chest, face, and so forth. This may happen before, during or soon after birth (up to two years of age approximately), when it is known as congenital hemiplegia (or unilateral cerebral palsy), or later in life as a result of injury or illness, in which case it is called acquired hemiplegia. Generally, injury to the left side of the brain will cause a right hemiplegia and injury to the right side a left hemiplegia.
Hemiplegia is a condition which is lifelong and non-progressive, that is they do not get worse.
How does hemiplegia occur?
Acquired hemiplegia results from brain injury. The most common cause is a stroke (when a bleed or blood clot damages part of the brain), but it can also result from a head injury or infection.
What are the effects of hemiplegia?
It is difficult to generalise: hemiplegia affects each person differently. The most obvious result is a varying degree of weakness, stiffness (spasticity) and lack of control in the affected side of the body, rather like the effects of a stroke. In one person this may be very obvious (he or she may have little use of one hand, may limp or have poor balance); in another person it will be so slight that it only shows when attempting specific physical activities.
What can be done to help?
Hemiplegia cannot be cured, but a lot can be done to minimise its effects and help the individual achieve their potential. The person, once diagnosed, will probably be referred to a rehabilitation department of your local or regional hospital. Therapists, who work as part of a wider network of professionals including neurologists and orthopaedic and neurosurgeons, will work in partnership with you to develop his or her abilities.
Understanding hemiplegia and knowing how you can help your loved one achieve his or her potential is vital.
Your loved one’s management will probably be based on a multidisciplinary approach, involving physiotherapy, occupational therapy, and possibly speech therapy where required. A physiotherapist and often an occupational therapist will work closely with each other and with partners or carers, to agree a programme of management with specific goals that are tailored to your loved one’s development and needs. The aim will be to improve their participation in everyday activities e.g. social activities, feeding, dressing, and toileting. The therapists will work to develop their skills, assessing posture and providing muscle stretching, and possibly strengthening activities. This will help prevent possible secondary consequences of the condition such as pain or the development of weakened muscles.
Goals could include improving function so that your loved one can grasp an object with the affected hand, or walk better. They should take into account the partner/ carers’ views, the time and effort involved in carrying out therapy activities, the impact on the patient and his/her family and how effective the activities might be.
A therapy programme will probably include training partners/carers, and later the induvial him/herself, to carry out exercises or techniques which they should continue to use at home, e.g. during dressing or bathing, so that they become part of the individual’s everyday life. The person’s progress should be reviewed regularly to assess how well the therapy programme is working and consider whether there is a need for other treatments as well. These might include orthoses (devices, such as splints, fitted to the body to improve posture and/or function); medications or orthopaedic surgery.
In general the person with hemiplegia should be treated as normally as possible. It is essential to involve the affected side in everyday activities, to make your loved one as “two-sided” as he or she can be.
Are there other problems associated with hemiplegia?
Yes, there may be. Because hemiplegia is caused by injury to the brain, it is not just motor pathways and motor development that may be affected. And despite the developing brain’s effort to relocate functions to undamaged areas, additional diagnoses may occur. Some of these are medical in nature, such as epilepsy, visual impairment or speech difficulties. Many people have less obvious additional challenges, such as perceptual problems, specific learning difficulties or emotional and behavioural problems. Each patient should be fully assessed and regularly monitored to identify if any of these associated problems are present.
What does the future hold?
In merely defining hemiplegia with its causes and effects we leave out perhaps the most important issue – the shock of diagnosis and the fear of the unknown. When a person is first diagnosed, it is often difficult for a doctor to predict whether problems will be mild or severe later in life. He or she will often adopt a ‘wait and see’ approach, which the patient and their supporters may find difficult to accept, since they may feel they are not being given all the facts. Understanding hemiplegia and knowing how you can help your loved one achieve his or her potential is vital. Make good use of the specialists dealing with your loved one’s hemiplegia. Do ask them questions and make sure you understand their replies, if necessary asking them to repeat them using non- specialist terms.
Support
Life can be difficult for someone with hemiplegia who want to do the same things as they previously did. They tire more easily and the effort involved in simple tasks can be considerable. They need all the help and encouragement you can give them. And you need support in your turn – ideally from others who understand how you feel and with whom you can also share ideas and information.
You may find general support groups for disabled patients and their families in your own area – your hospital or library should have information. And you may want to a national organisatio
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal